Injury Recognition: Ankle Tests
This is an excerpt from Examination of Musculoskeletal Injuries 4th Edition With Web Resource by Sandra Shultz,Peggy Houglum & David Perrin.
Injury Recognition and Special Tests
The majority of active people experience leg and foot problems sometime in their lives. Tremendous forces, both compressive and rotational, are transmitted through the weight-bearing structures of the foot, ankle, and leg. Consequently, both traumatic and chronic injuries frequent this region. Even seemingly minor injuries can be debilitating given the foot and ankle's need for strength and stability in daily weight-bearing activities, let alone sport activities. Additionally, leg and foot problems can alter gait or lower-body mechanics, increasing stress and compensatory problems up the kinetic chain in the knee, hip, or low back.
Acute Soft Tissue Injuries
The leg complex relies on the integrity of active and passive soft tissue structures for both stability and propulsion. Dynamic sport activity places tremendous loads and demands on the foot and ankle. Soft tissue injuries commonly occur as a result of direct contact and intrinsic or extrinsic forces acting on the foot, ankle, and leg.
Contusions
Making contact with the ground or an opponent, kicking an unyielding object, being hit in the shin by a baseball, and being stepped on or kicked by another player are all common injury mechanisms for soft tissue and periosteal contusions. Signs and symptoms include pain, swelling, and discoloration. Direct contact to the superficial and unprotected anterior medial border of the tibia can result in localized inflammation (periostitis) and hematoma formation under the periosteum, which can take considerable time for the body to absorb. Disability and function loss are usually more severe with muscle contusions as a result of tenderness, swelling, and spasm within the muscle tissue. Decreased range of motion and strength also occurs and varies according to the degree of tissue injury. Although muscle contusions rarely result in serious injury, complications can arise from severe contusions and excessive bleeding within the enclosed anterior tibial compartment of the leg (see the discussion of anterior compartment syndrome earlier in this chapter). You should closely monitor contusions that result in severe swelling of a muscular compartment for neurovascular compromise.
You should closely monitor severe contusions to a muscular compartment for excessive swelling and neurovascular compromise.
A heel contusion, or stone bruise, can be particularly problematic. A heel bruise can result from landing hard on the heel during jumping activities or stepping on an uneven surface or a stone at heel strike with little or no footwear protection. A contusion to the fat pad of the heel can cause considerable pain and point tenderness, making it difficult to bear weight or walk with a normal gait. Discoloration and swelling may or may not be evident, depending on severity.
Sprains
The foot and ankle include multiple joints and ligaments that stabilize the body during weight-bearing activities. Given the tremendous forces exerted on these structures during landing, cutting, and running, the ligaments are prone to injury when these forces extend the joint beyond its normal ROM. Sprains occur most often at the hindfoot, which is composed of the inferior tibiofibular (syndesmosis), talocrural (tibia, fibula, and talus), and subtalar (talus, calcaneus, navicular) joints. Ligamentous support is essential for stabilizing the hindfoot, particularly when the ankle plantar flexes. Stability is provided medially by the deltoid ligament complex (refer to figure 16.2) and laterally by the anterior talofibular, calcaneofibular, and posterior talofibular ligaments (refer to figure 16.3). The distal tibiofibular joint is stabilized by the interosseous membrane and the anterior and posterior tibiofibular ligaments. Although sprains occur most often at the hindfoot, sprains in the midfoot (talocalcaneonavicular, cuneonavicular, intercuneiform, and calcaneocuboid joints) and forefoot(tarsometatarsal, intermetatarsal, metatarsophalangeal, and interphalangeal joints) are not uncommon. The injury mechanism determines which joint structures are involved.
Lateral Ankle Sprains
The most common mechanism of ankle injury involving the lateral ligament complex is inversion with or without plantar flexion. In typical scenarios, a basketball player comes down on an opponent's foot or lands awkwardly on the outside of his own foot, causing the ankle to turn in (inversion mechanism). The athlete complains of immediate pain upon injury and may hear a pop. Injury almost always involves the anterior talofibular ligament (figure 16.22). The calcaneofibular and, less often, the posterior talofibular ligaments are also involved. Signs and symptoms are consistent with first- through third-degree ligament sprains. However, remember that the amount of swelling is a poor indicator of injury severity with lateral ankle sprains because even minor sprains can result in considerable joint swelling. With second- and third-degree sprains, there may also be injury to the medial structures of the ankle as a result of compression from the inversion force. Dislocation of the ankle mortise rarely results with third-degree ligament injuries, but associated avulsion or push-off fractures of the lateral and medial malleolus, respectively, are not uncommon with more severe ankle sprains. Because of this, you must be able to distinguish between soft tissue and bony tenderness during palpation. To test the integrity of the lateral ligament complex, use the anterior drawer test to examine both the anterior talofibular and calcaneofibular ligaments, and the medial talar tilt (inversion stress) testto primarily test the calcaneofibular ligament. An alternative testing position for the anterior drawer test is with the patient prone and the foot hanging off the edge of the table. Place one hand under the distal anterior surface of the tibia and apply an anteriorly directed force to the calcaneus.

Injury to the lateral ligaments of the ankle.
Anterior Drawer Test

Other names for test
None
Used to assess
Integrity of anterior talofibular ligament and calcaneofibular ligament
Patient position
Either long-sitting or supine, knee slightly flexed to relax the gastrocnemius, and ankle in 20° plantar flexion
Clinician position
Standing at foot of table
Clinician's stabilizing hand position
Stabilizing distal tibia and fibula just above malleoli
Clinician's test hand position
Grasping calcaneus posteriorly
Action performed
Pull calcaneus forward on talus.
Positive result
Pain and laxity; laxity is greater when both ligaments are torn.
Accuracy
- SN = .58-.83 SP = .38-1.0 +LR = 1.2-2.2 - LR = 0.39-0.70
Croy et al. 2013; Raatikain, Putkonen, and Puranen 1992; Van Dijk et al. 1996.
Medial Talar Tilt Test

Other names for test
Inversion (varus) stress test
Used to assess
Integrity of calcaneofibular ligament
Patient position
Either long-sitting or supine
Clinician position
Standing at foot of table
Clinician's stabilizing hand position
Stabilizing medial distal leg just above medial malleolus
Clinician's test hand position
Grasping lateral foot along calcaneus to hold ankle in anatomical neutral position
Action performed
Adduct and invert calcaneus.
Positive result
Pain and laxity
Accuracy
- SN = .50 SP = .88 +LR = 4.00 - LR = 0.57
Hertel et al. 1999; Schwieterman et al. 2013.
Medial Ankle Sprains
Medial ankle sprains resulting from eversion forces are considerably less common, primarily because of the greater stability of the medial ankle, a consequence of the thickness and strength of the deltoid ligament complex as well as the longer lateral malleolus, which prevents excessive eversion (figure 16.23). Palpate the distal fibula for possible fracture with severe eversion injuries. Signs and symptoms are consistent with first-, second-, and third-degree sprains. To test deltoid ligament integrity, use the lateral talar tilt (eversion stress) test and Kleiger (lateral rotation) testto determine the degree of instability. Disability and recovery may be prolonged with medial ankle sprains; given the support the deltoid ligament provides to the medial longitudinal arch of the foot, even simple weight-bearing stresses the injured structures. Furthermore, pes planus and excessive pronation may result from chronic medial instability.
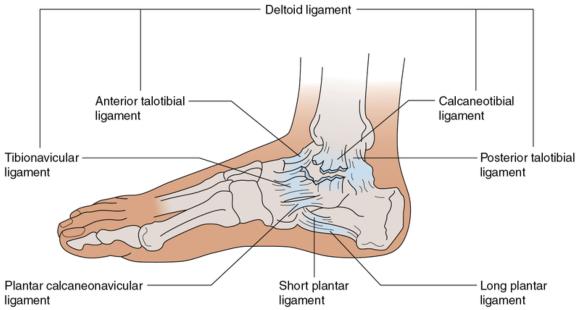
Injury to medial ligaments of the ankle. Carefully palpate the distal fibula for possible fracture with all serious eversion injuries.
Lateral Talar Tilt Test

Other name for test
Eversion (valgus) stress test
Used to assess
Integrity of deltoid ligament
Patient position
Either long-sitting or supine
Clinician position
End of table, facing patient
Clinician's stabilizing hand position
Stabilizing lateral distal leg with hand over lateral leg proximal to lateral malleolus
Clinician's test hand position
Grasping medial calcaneus and positioning ankle in neutral
Action performed
Abduct and evert the calcaneus.
Positive result
Pain and laxity
Accuracy
- SN = N/A SP = N/A +LR = N/A - LR = N/A
Kleiger Test

Other name for test
Lateral rotation test
Used to assess
Integrity of deltoid ligament
Patient position
Sitting, knee flexed to 90° and foot relaxed
Clinician position
Standing at foot of table
Clinician's stabilizing hand position
Stabilizing leg by grasping distal tibia and fibula
Clinician's test hand position
Grasping top of metatarsal region of foot
Action performed
Rotate the foot laterally.
Positive result
Medial ankle pain with or without laxity (talar displacement)
Accuracy
- SN = N/A SP = N/A +LR = N/A - LR = N/A
SHOP

Get the latest insights with regular newsletters, plus periodic product information and special insider offers.
JOIN NOW
Latest Posts
- What’s it like to use the School Wellness Education model with Grades 5 and 6?
- Clarifying what you are teaching and building relevance for students
- What is the School Wellness Education model?
- Understanding Facility Use and Users’ Needs in Designing Esports Spaces
- 6 Types of Esports Games
- Esports Career Pathways