Intellectual Disability: Adaptive Functioning and Levels of Support
This is an excerpt from Adapted Physical Activity Across the Life Span by Carol Leitschuh,Marquell Johnson.
How a person with an ID managed their life was ignored when IQ was the sole emphasis in diagnosis. The AAIDD fought to have an assessment of adaptive functioning added to the determination of ID to clearly identify the supports needed to meet determined societal expectations to manage life. The AAIDD has defined adaptive behavior (see sidebar) and laid out levels of support within those behaviors (Schalock et al., 2010).
Adaptive Behavior Defined by the AAIDD
Adaptive behavior is the collection of conceptual, social, and practical skills that are learned and performed by people in their everyday lives.
- Conceptual skills: These include language and literacy; money, time, and number concepts; and self-direction.
- Social skills: These include interpersonal skills, social responsibility, self-esteem, gullibility, naïveté (i.e., wariness), social problem-solving, and the ability to follow rules and obey laws and to avoid being victimized.
- Practical skills: These include activities of daily living (personal care), occupational skills, seeking and receiving healthcare, conducting travel, maintaining schedules, being safe, using money, and using the telephone.
From: American Association on Intellectual and Developmental Disability (AAIDD). Available: www.aaidd.org/intellectual-disability/definition.
Regarding adaptive functioning, it is understood that expectations vary for different age groups. During infancy and early childhood, significant delays in motor skills, communication skills, self-help skills, and sensory-motor activities are potential indicators of ID. During childhood and early adolescence, the primary focus is on the ability to learn basic academic skills, which includes physical education. As the student enters high school ages, a gradual focus shifts to making a living and to handling oneself and one’s affairs. What level of support is needed in what areas? Is it continuous or is it episodic?
The Diagnostic Adaptive Behavior Scale is an assessment tool for individuals ages 4 to 21 years (Tassé et al., 2016). This tool aligns perfectly with the adaptive skills advocated for assessment by the AAIDD. These adaptive skills are listed for conceptual, social, and practical skills in the sidebar. An individualized education program (IEP) for a four- or five-year-old will address social skills and will address practical skills related to personal care (use of the bathroom and handwashing) often expanding on those skills emergent in the earlier individualized family service plan (IFSP).
The Vineland Adaptive Behavior Scales, Third Edition (Sparrow et al., 2016) is another standardized tool for assessing adaptive functioning. Used with individuals from birth to age 90, the tool assesses communication and daily living. Many of these assessment results find their way into the IFSP for the youngest children and the IEP for those aged at least into first grade.
The AAIDD has assessment tools for determining the level of support required for a child or an adult to be successful in the home and community (Thompson et al., 2002). Supports Intensity Scale-Children’s Version (AAIDD, 2016) is appropriate for ages 5 to 16. In part I of the tool, focus is on specific medical conditions and behavioral concerns potentially requiring support. Part II assesses activities for home living, community and neighborhood, school participation, school learning, health and safety, social activities, and advocacy. The adult version of the scale (AAIDD, 2015) measures support needed for success in home living, community living, lifelong learning, employment, health and safety, social activities, and protection and advocacy.
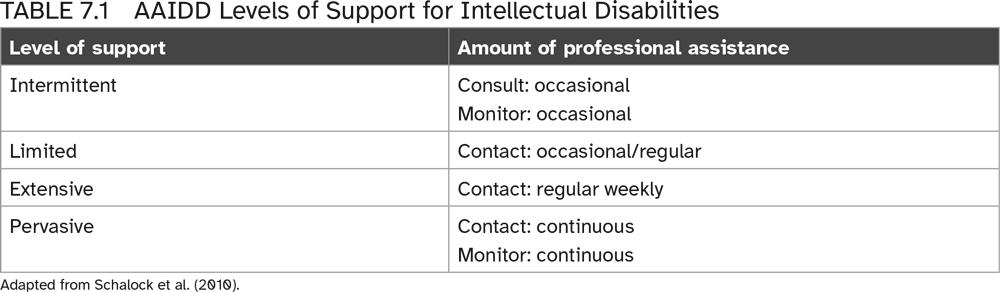
The levels of support are used in APE and GPE environments to distinguish what is needed for the student with ID to learn. The support level runs on a continuum from intermittent to pervasive, from settings that are selective to nearly all settings, and with varying amounts of professional assistance. Table 7.1 is, therefore, a necessary guide to apply to the implementation of an IEP in the student’s physical education placement.
The relationship between a deficit in adaptive function and the support needed (table 7.1) is critical to understand. Effective matching of these realities equals program engagement in physical activity for the student with ID.
SHOP

Get the latest insights with regular newsletters, plus periodic product information and special insider offers.
JOIN NOW
Latest Posts
- Physician supervision in pulmonary rehabilitation programs
- Patient centered outcomes for pulmonary rehabilitation programs
- Positioning pulmonary rehabilitation within the GOLD 2025 guidelines
- Issues with ratios in statistical analysis in kinesiology
- Factorial ANOVA: Within-within example
- How to calculate skewness and kurtosis